Electrodiagnostic (EDX) studies are a commonly used technique to test the function of muscles and nerves.
Electromyography & nerve conduction study

Definition
Electromyography (EMG) is an electrical recording of muscle activity that aids in the diagnosis of neuromuscular disease.
Purpose
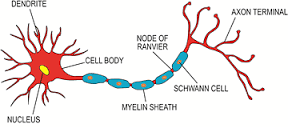
Muscles are stimulated by signals from nerve cells called motor neurons. This stimulation causes electrical activity in the muscle, which in turn causes contraction. This electrical activity is detected by a needle electrode inserted into the muscle and connected to a recording device. Together, the electrode and recorder are called an electromyography machine. EMG can determine whether a particular muscle is responding appropriately to stimulation, and whether a muscle remains inactive when not stimulated.
EMG is performed most often to help diagnose different diseases causing weakness. Although EMG is a test of the motor system, it may help identify abnormalities of nerves or spinal nerve roots that may be associated with pain or numbness. Other symptoms for which EMG may be useful include numbness, atrophy, stiffness, fasciculation, cramp, deformity, and spasticity. EMG results can help determine whether symptoms are due to a muscle disease or a neurological disorder, and, when combined with clinical findings, usually allow a confident diagnosis.
EMG can help diagnose many muscle and nerve disorders, including:
- muscular dystrophy
- congenital myopathies
- mitochondrial myopathies
- metabolic myopathies
- myotonias
- peripheral neuropathies
- radiculopathies
- nerve lesions
- amyotrophic lateral sclerosis
- polio
- spinal muscular atrophy
- Guillain-Barré syndrome
- ataxias
Description
- Donuring an EMG test, a fine needle is inserted into the muscle to be tested. This may cause some discomfort, similar to that of an injection. Recordings are made while the muscle is at rest, and then during the contraction. The person performing the test may move the limb being tested, and direct the patient to move it with various levels of force. The needle may be repositioned in the same muscle for further recording. Other muscles may be tested as well. A typical session lasts from 30-60 minutes.
Normal results
There should be some brief EMG activity during needle insertion. This activity may be increased in diseases of the nerve and decreased in long-standing muscle disorders where muscle tissue is replaced by fibrous tissue or fat. Muscle tissue normally shows no EMG activity when at rest or when moved passively by the examiner. When the patient actively contracts the muscle, spikes (motor unit action potentials) should appear on the recording screen, reflecting the electrical activity within. As the muscle is contracted more forcefully, more groups of muscle fibers are recruited or activated, causing more EMG activity.
Abnormal results
The interpretation of EMG results is not a simple matter, requiring analysis of the onset, duration, amplitude, and other characteristics of the spike patterns.
Electrical activity at rest is abnormal; the particular pattern of firing may indicate denervation (for example, a nerve lesion, radiculopathy, or lower motor neuron degeneration), myotonia, or inflammatory myopathy.
Decreases in the amplitude and duration of spikes are associated with muscle diseases, which also show faster recruitment of other muscle fibers to compensate for weakness. Recruitment is reduced in nerve disorders.
nerve conduction study

The routine NCS includes testing of the motor and sensory fibers of the median, ulnar and radial nerves, the motor fibers of the peroneal and tibial, and the sensory fibers of the superficial peroneal and sural nerves. Less frequently, the facial and the accessory nerves are tested. While the typical NCS tests the distal nerve, the late responses, H-reflexes and F-wave latencies, provide information about the proximal segment.
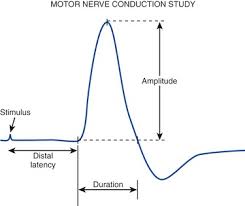
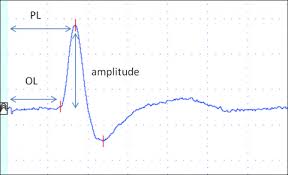
In motor NCSs, the nerve is stimulated at least at two points along its course. Supramaximal stimulation ensures the activation of all axons. The active surface electrode is placed on the muscle belly innervated by the nerve while the reference electrode is positioned distally on the tendon. The waveform is called compound muscle action potential (CMAP). The stimulus is delivered at increasing distances from the muscle. Parameters measured include latency from the stimulus artifact to the onset of the negative response, amplitude from the baseline to the negative peak and motor conduction velocities (CV).
The electrodes in sensory NCSs are attached over a sensory or a mixed nerve. The
stimulation can be proximal (antidromic) or distal (orthodromic) to the recording electrode. It is more challenging to obtain the sensory nerve action potential (SNAP). Latency, amplitude and sensory CV are usually measured. Stimulation at different sites along the nerve results in change of the waveform and temporal dispersion that is important to recognize.
Questions answered
EMG and NCS play a very important role in the evaluation of patients presenting with neuromuscular problems. When used in conjunction with a thorough neurological history and examination, they provide critical information that guides further laboratory testing, medical or surgical management. Furthermore, the EDX should be individualized depending on the findings. NCS and EMG are predominantly used for evaluation of peripheral nervous system, including motor neuron, dorsal root ganglion, root, plexus, nerve, neuromuscular junction and muscle diseases. The studies provide the following important information:
Localization within the neuromuscular system. EDX is helpful to distinguish if the problem is related to a single nerve (mononeuropathy), several nerves (multifocal neuropathy or polyneuropathy), one or more nerve roots (monoradiculopathy or polyradiculopathy), plexus (plexopathy), anterior horn cell (motor neuronopathy) or dorsal root ganglion cell (sensory neuronopathy). Muscle and NMJ diseases are also diagnosed with a good degree of certainty. The exact localization is sometimes difficult to determine clinically. For example, in a patient presenting with a foot drop, the problem could be due to motor neuron disease, lumbo-sacral radiculopathy or peroneal neuropathy. The NCS and needle EMG help in establishing the origin of the problem and guide further evaluation. MRI of the lumbar will not be indicated in a case of peroneal entrapment at the fibular head. On the other hand, absence of entrapment, normal SNAPs and denervation changes in L4-5 root distribution will point to radiculopthy and imaging study will be necessary. Finally, normal SNAPs, decreased or normal CMAP amplitudes and widespread denervation changes will lead diagnosis of motor neuron disease.
Fiber type involvement. In neuropathic diseases, EDX gives insight on the affected fiber types, motor, sensory or both. Sensorimotor polyneuropathies are quite common. However, if the study demonstrates only sensory or motor neuropathy, the differential diagnosis becomes more limited. Sensory NCSs are abnormal in lesions of the dorsal root ganglion, plexus or peripheral nerve. They are normal in disorders of the muscle, NMJ, root and motor neuron. Patients with ventral root lesions frequently have subjective sensory symptoms but the sensory nerve studies remain normal, since the dorsal root ganglion remains intact. Patients with small fibers neuropathy have normal sensory nerve studies despite the sensory symptoms that they have. In disorders of the muscle, NMJ, ventral root and the anterior horn cell, the CMAPs are abnormal, while the SNAPs are spared.
Underlying pathophysiology. The EDX can determine the type of abnormality, demyelination or axonal loss. The two can co-exist. Criteria for demyelination in the motor nerves include increased distal motor latency, slowing of the CV to less than 80 percent of the normal, conduction block and increased temporal dispersion. The conduction block is a result of a failure to activate the next node of Ranvier. In the sensory nerves, slowing of the CV is consistent with demyelination. The nerve is considered demyelinated if at least one of the above criteria is met.8 In a focal process, as in carpal tunnel syndrome, the findings are limited only to one nerve. Multiple nerve involvement can be seen in the demyelinating polyneuropathies.
On the other hand, axonal loss causes reduction of the SNAP and CMAP amplitudes, the severity of which depends on the extent of the axonal damage. Mild slowing of the CVs also occurs but it does not reach the decrease seen in the demyelinating cases. The earliest sign of axonal loss on needle examination is decreased recruitment, followed by appearance of fibrillation potentials and positive waves within one to three weeks. Features of reinnervation, large MUPs with high amplitude, appear within several months. For determining the type of polyneuropathy, most protocols require testing of the sensory and motor nerves in at least two extremities. The majority of the polyneuropathies are axonal and the differential diagnosis is broad, while the number of primary demyelinating polyneuropathies is very limited. In the acquired demyelinating polyneuropathies, the demyelination is patchy and conduction block is a common finding. A few examples of common demyelinating polyneuropathies for which there are available therapies include chronic inflammatory demyelinating polyneuropathy (CIDP), acute inflammatory demyelinating polyneuropathy (AIDP of Guillaine-Barre syndrome) and multifocal polyneuropathy (MMN). The hereditary types are characterized by uniform changes and can be confirmed by genetic testing.
Severity of the disease and prognosis for recovery. The studies can also measure the severity and prognosis for recovery of the following:
Traumatic nerve injury.
EDX provides valuable information about prognosis in traumatic nerve injury. Neuropraxic injury presents with conduction failure without axonal degeneration and carries best prognosis for recovery. Axonotmesis and neurotmesis affect the axon and can not be differentiated during the initial study. Decrease of the CMAP amplitude confirms axonal damage. Needle EMG detects denervation of muscles that do not seem to be clinically affected. However, it may show residual innervation to paralyzed muscles. The optimal time to search for denervation changes is 10 to 14 days after the injury. Follow-up EMG studies may demonstrate early reinnervation with appearance of nascent MUPs that may further increase in amplitude which is accompanied by increase of CMAP amplitudes with continuous improvement Sensory studies are less helpful in evaluating axonal regeneration. Absence of regeneration three to four months after the injury requires surgical exploration. Traumatic root avulsion and brachial plexopathy could be differentiated using EDX. The clinical significance is that the former condition precludes surgical intervention. Normal SNAPs in the presence of dermatomal sensory findings and denervation in myotomal distribution is the strongest evidence that favors root avulsion. Denervation of the paraspinal muscles lacks sensitivity.
Facial neuropathy

EDX can estimate the severity and prognosis of patients with facial neuropathy. CMAP amplitude compared to the contralateral side is the best parameter, but there is no reliable technique to evaluate patients in the first 24-48 hours. The optimal time for EDX study is at least five to eight days after onset. Needle EMG has little prognostic value. However, detecting MUPs in a paralyzed muscle is consistent with better prognosis. CMAP latency and blink reflex have not been found useful.
Radiculopathy
EMG and NCSs have little prognostic value in radiculopathy when compared to clinical and psychosocial factors. These studies are used mostly in evaluating for presence of a superimposed process such as polyneuropathy.
Mononeuropathy


Focal neuropathies, carpal tunnel syndrome (CTS) and ulnar neuropathy are precisely evaluated with NCS. The severity of CTS is graded based on changes of the sensory and motor potentials, which aids in determining the need for surgery. The NCSs improve with therapeutic interventions for carpal tunnel syndrome, including splinting, steroid injections and surgery. Ulnar neuropathy at the elbow and peroneal neuropathy at the fibular head are also localized with these studies but their correlation with clinical improvement after surgery is less well established.
Neuropathy.
NCSs do not contribute significantly in the prognosis of the axonal polyneuropathies. However, studies have shown a role in evaluating the response to therapy in diabetic polyneuropathy. Similarly, follow-up studies demonstrate recovery from toxic, alcohol-related and nutritional neuropathies. In severe cases of AIDP, axonal damage develops in addition to the demyelination that is the rate limiting factor for recovery. With few exceptions, the distal CMAP amplitude of the peroneal, tibial, median and ulnar nerves has been found to be the most powerful predictor for prognosis. Use of EDX in prognostication of CIDP is more difficult due to the complexity of the natural course of the disease. The degree of axonal damage determines the prognosis. Improvement of the conduction velocity and CMAP amplitude has been used to demonstrate improvement in clinical trials. Secondary axonal loss during the course of severe and long standing focal demyelination is associated with worse prognosis. For instance, compression of the median nerve in the carpal tunnel causes focal demyelination. If prolonged, axonal loss develops that can result in loss of strength and muscle bulk of the thenar muscles and is associated with incomplete or absent recovery.
Neuromuscular junction disorders
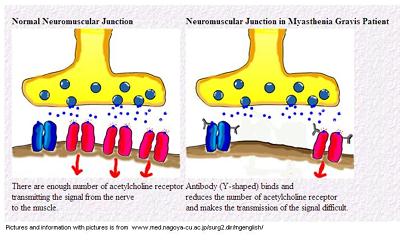
SFEMG abnormalities show good correlation with muscle strength in patients with myasthenia gravis (MG). It also provides predictive value for worsening and improvement of the condition. It can be abnormal in patients with no clinical weakness. RNS is much less sensitive and is normal in remission. Abnormal decrement is more likely in generalized than in ocular MG. EDX has most value in management of patients with LEMS by following the response to treatment. SFEMG and CMAP amplitude are of highest importance, followed by percentage of CMAP facilitation and decrement at low-rate RNS.
Muscle disease
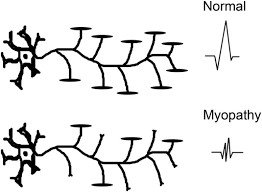
Small, brief and polyphasic MUPs, as well as fibrillation potentials, positive waves and complex repetitive discharges are frequently seen in patients with inflammatory myopathies. The presence of spontaneous activity is a measure of response to treatment. Fibrillation potentials and positive waves are found in other myopathies associated with muscle fiber necrosis. In patients with inflammatory myopathies treated with steroids, detecting fibrillation potentials and positive waves in weak muscles means that the disease is not adequately treated, while absence of such activity indicates that the steroid dose should be reduced. In patients with inflammatory myopathies, the abnormal EMG in weak muscle serves as a guide for a good muscle biopsy site. It is important to remember that a muscle that is recently studied by a needle EMG should not be used for biopsy, since the changes can mimic myositis.
Instead, the contralateral muscle could be subjected to biopsy because of the disease symmetry. The availability of genetic testing has replaced to a great extent the use of needle EMG in the diagnosis of the hereditary muscle disorders. Critical illness myopathy presents with variable degree of reduction of the CMAPs. The EMG changes do not always correlate with the degree of weakness and the prognosis.
Motor neuron disease
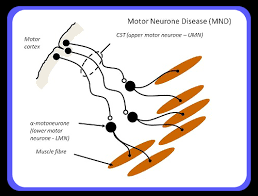
EDX contributes to the identification of the lower motor neuron involvement in amyotrophic lateral sclerosis (ALS), sometimes even before the clinical manifestation. One of the primary findings is decreased recruitment. Asynchronous firing results in increase in polyphasic MUPs. The most reliable abnormality is the fibrillation potentials and positive waves. Their abundance does not correlate with disease progression. The presence of increased in amplitude and duration MUPs is an indicator for collateral sprouting and reinnervation. The irritability of the lower motor neuron manifests with appearance of fasciculations that are not specific for ALS. For definite diagnosis, decreased recruitment, fibrillation potentials and large MUPs have to be identified in at least three levels of the neuraxis (bulbar, cervical, thoracic or lumbar). Clinically weak muscles, innervated by different roots and peripheral nerves must be selected. NCSs are important to exclude mimickers of ALS, such as MMN, radiculopathy, mononeuropathy, polyneuropathy and others. ALS patients have normal sensory studies unless there is an underlying problem. Another typical finding that correlates with the prognosis but lacks sensitivity is the decrease of the CMAP amplitude. The time to death is best judged based on a combination of clinical and EMG findings.Motor unit number estimation (MUNE) has value in following the disease progression since it measures more objectively the number of the remaining anterior horn cells. However, its use is limited to specialized laboratories.
Temporal Course of Disease
EDX studies provide information on the course of the nerve disease that can be hyperacute (one week), acute (a few weeks), subacute (a few weeks to a few months) or chronic (months to years). The decision on the timing of the lesion requires careful analysis of the history and the findings on the examination. Studies on transected nerves demonstrate that it usually takes between three to five days for the Wallerian degeneration to result in a drop of the CMAP with maximum decrease at around day seven and nine. Lower amplitudes of the SNAP may first be seen between day five and seven with maximal decrease at days 10 to 11. Decrease of the CMAP amplitudes is an early sign of axonal injury but EMG has a greater role in testing muscles that can not be evaluated by NCS. The earliest sign is decreased recruitment. Fibrillation potentials start developing within days after the injury with a best yield achieved two to three weeks post injury. Therefore, the ideal time to perform EDX is after day 10. But if GBS is suspected, the study should not be postponed.
Important Considerations
The EDX must be done in conjunction with a careful neurological history and examination. The study should be tailored depending on the differential diagnostic possibilities. When the examination and the EDX findings are conflicting, the examiner should re-evaluate the patient and consider the possibility of a technical problem. For instance, if a patient has normal sensory examination and Achilles tendon reflexes, the absent H-reflexes should raise a question about a technical factor.
The patient needs to be informed about the nature of the test. Many fear the study based on rumors that the study is very painful and difficult to tolerate. Others ask if pain medication are needed prior to the testing. In reality, there is discomfort with the electrical stimulation and pain with needle examination.
Pain could be a significant limiting factor. In our own and other investigators’ experience, caring approach, explaining the procedure and distracting the patient during the procedure are important determinants of pain perception. Pain medications are not recommended prior to the test. Age, gender, primary symptoms, previous EMG and time of the needle within the muscle are not related to the level of discomfort. Some studies find no relation between needle types. Others demonstrate that monopolar needles are associated with less pain, but using concentric needle with small movement technique leads to similar result. If the patient still has trouble tolerating the procedure, the examiner should start with the area of greatest interest.Starting with testing of the sensory nerves could be preferable, since they require lower electrical stimulus. The patients are more likely to tolerate higher stimulation to achieve a supramaximal response or multiple redirections of the needle during EMG when they understand the reason for it.
Technical Factors
Physiologic factors. The most important physiologic factor is the temperature. The effect of the skin temperature on the CV and distal latency is well documented.Optimally, the room should have a local temperature control. The temperature of the extremities is monitored with a probe. The general rule is that the hand temperature should be >33°C and that of the foot >31°C. If suboptimal, the extremities have to be warmed up using heating pads, a lamp, or warm water. The examiner must know that with every 1°C drop of the temperature, the motor and sensory CV decreases between 1.5 and 2.5 m/s, and the distal latency becomes prolonged by 0.2 ms. In addition, the amplitude of the SNAP and CMAP may increase. When the temperature is suboptimal, the MUPs become polyphasic, with longer duration and higher amplitudes. Slowing of the nerve CVs in a person with cold extremities may lead to wrong diagnosis of peripheral neuropathy and unnecessary testing. Other physiological factors that need attention are age, height and anomalous innervation. Edema, skin lesions, and obesity are limiting factors in performing a successful EDX study.
Non-physiological factors. It is imperative to understand the need for supramaximal stimulation when performing NCSs. Limb positioning with obtaining measurements is of importance too, particularly in the case of the ulnar nerve where the elbow must be flexed from 70-90°. This position provides the best correlation between the surface measurement and the length of the nerve. Proper placement of electrodes, correct measurements, and using appropriate distance between the active and reference electrodes are a few of the other non-physiological factors. The electromyographer should be able to recognize artifacts. Common errors are submaximal stimulation and improper placement of the electrodes, which may result in lower amplitudes of the nerve potentials leading to an incorrect assumption that the patient has axonal loss. Submaximal stimulation of deeply located nerves—for example, ulnar nerve below the elbow— may give an erroneous impression of a conduction block. On another hand, high stimulus may co-stimulate neighboring nerves. This phenomenon is difficult to avoid with proximal stimulation in the axilla. The examiner has to observe the shape, amplitude, and latency of the responses that should not change significantly. Ambient noise can be an obstacle in obtaining sensory responses, particularly in the ICU.7 Failure to recognize technical factors of errors could lead to unnecessary testing, treatment and even surgery.
Bleeding Complication
Although rare, bleeding is a potential complication with needle EMG. Since this is an invasive procedure, the risk theoretically increases with the use of anticoagulation, antiplateletes, NSAIDs, and herbals with mild anticoagulation properties (e.g. Ginko biloba, Ginseng, Saw Palmetto, and others). Thrombocytopenia below 50,000/mm3, platelet dysfunction, and coagulopathies are related to higher risk for bleeding. The risk exists even in absence of anticoagulation. There are no guidelines to help the clinician handle patients with increased risk of bleeding. This may result in avoiding the procedure and cause delay in diagnosis.
There is a consensus that antiplatelet therapy is not associated with increased risk for hemorrhagic complications. Therefore, physicians are not required to stop antiplatelets prior to needle examination. Moreover, withholding antiplatelet therapy may increase the risk for cardiovascular and cerebrovascular events. Bleeding complications are low even in patients on anticoagulation. Studies do not demonstrate increased risk for clinically significant hematomas. The incidence of subclinical hematoma is very low, around 1.45 percent. There is no statistically significant increased rate of bleeding in patients with anticoagulation or antiplatelet therapy.
The electromyographer must use caution when performing needle examination on anticoagulated patients by using a smaller gauge needle and applying pressure for a longer period of time. It is better to avoid aggressive needle examination and deeper muscle testing particularly when hematoma can compress important structures. There is no recommended cut off INR for performing the needle examination. Some laboratories are comfortable with EMG of all patients with INR less or equal to 3.0, while patients with a higher INR are tested at the discretion of the electromyographer. The risks and benefits have to be weighed on a case-by-case basis when testing of anticoagulated patients.
Limitations
The EDX studies are normal in patients with small fiber peripheral neuropathy who present with burning pain and hypersensitivity. The study may not be revealing in some types of myopathy. As discussed above, the changes that occur with acute nerve injury take some time to develop. Therefore, the study may be negative if done very early and should be repeated if needed. In addition, EMG and NCSs are unlikely to be helpful in patients with generalized weakness, diffuse pain, or fatigue.
Conclusions
EMG and NCSs are valuable tools in the armamentarium of the physician dealing with patients with neuromuscular disorders. The test cannot be used in isolation and should be performed after a careful clinical examination. The clinical hypothesis determines the extent of the study performed and is tailored for each individual patient. Important information regarding localization, underlying pathophysiology, severity, temporal course and prognosis can be obtained. Further testing and treatment is provided depending on the underlying problem. The test has some limitations. If the EDX results and the clinical findings do not make sense, the patient has to be re-examined and technical factors must considered.
.